5 Pathology of the lens
The lens is a disc-like structure suspended by zonules at the posterior aspect of the anterior segment. It is avascular, and relies completely on the diffusion of nutrients from the aqueous humour. It’s deceptively simple appearance belies it’s important function: the refraction of light onto the retina to provide focus.
The lens is a living tissue, albeit a relatively simple one (See Figure 5.1). It is enclosed by the lens capsule, which is the basement membrane of the lens epithelial cells that make up the body of the lens. The capsule is impermeable to large proteins, but allows the entry of water and other nutrients, making the lens an immunologically privileged site. The lens epithelium lines the anterior half (and only the anterior half) of the lens capsule in a single, cuboidal layer. The lens epithelium is mitotically active, and continually divides to produce additional epithelial cells. These cells migrate centrally and elongate, forming the long fibers that make up the lens. As the epithelial cells differentiate, they lose their nuclei and organelles, forming the clear structure important to its function. Like the cornea, the lens maintains itself in a dehydrated state to help maintain its clarity; this is mediated by an active Na-K pump located on the anterior lens epithelial cells.
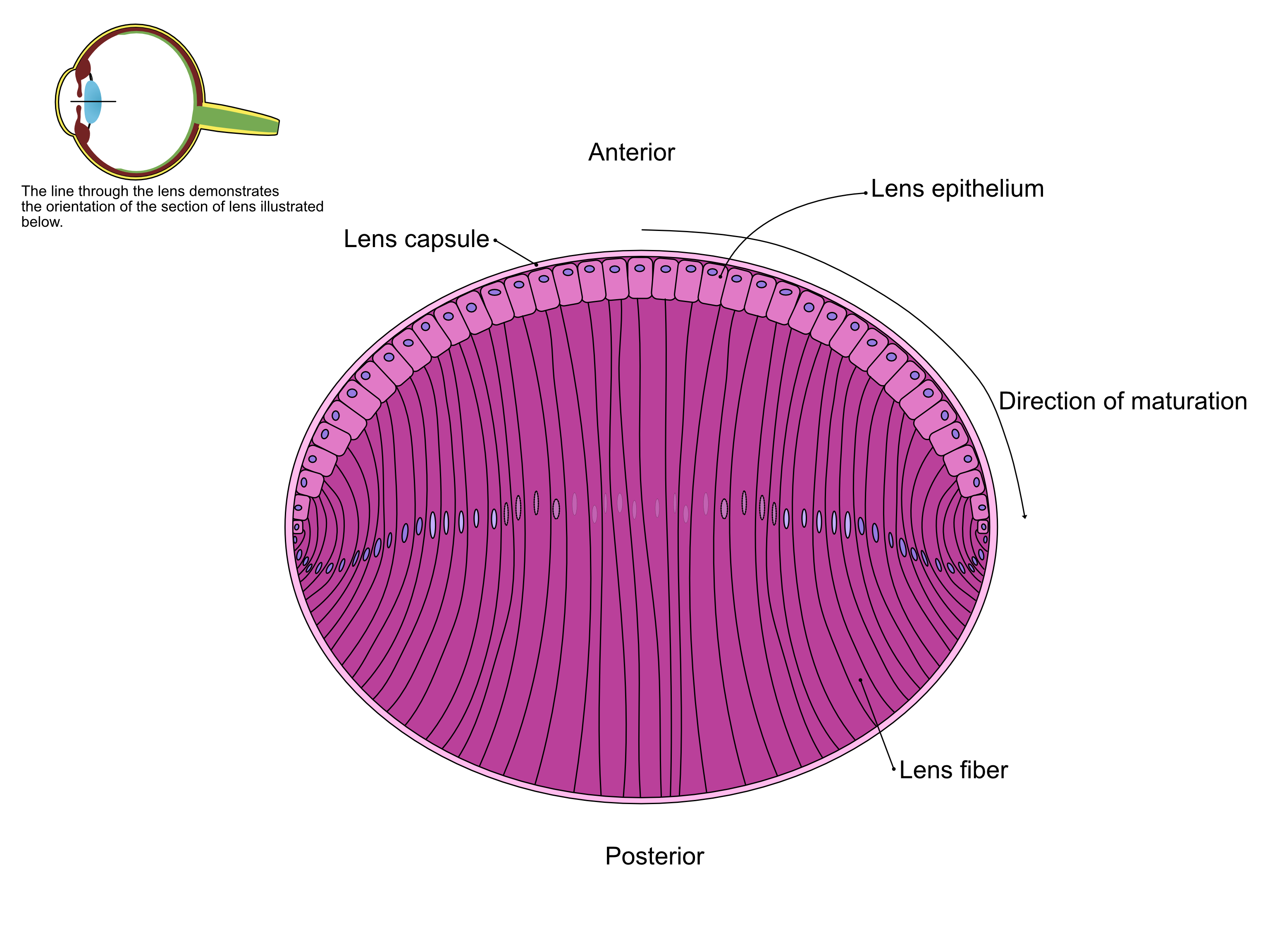
Figure 5.1: An anterior-posterior illustration of the lens, demonstrating the anterior epithelium, nuclear bow, lens capsule, and lens fibers.
The lens survives mainly on glucose delivered by the aqueous humour, which is metabolized via anaerobic glycolysis and the hexokinase pathway to produce energy. This small piece of information is a critical component to the understanding of the pathophysiology of cataracts.
5.1 Cataract
A cataract is defined as opacification of the lens. When severe, it is readily diagnosed on histopathology, however, ophthalmological exam is a far more sensitive and accurate method of diagnosing and describing cataracts.
The opacification of the lens is the result of alteration of the normally dehydrated lens and its well-organized lens fibers. In response to injury, the lens epithelium may attempt to proliferate, while lens fibers frequently undergo degenerative and hydropic changes. Proliferating epithelial cells may migrate to the normally acellular posterior aspect of the lens, contributing to opacity. The epithelial cells may also become hyperplastic along the anterior edge, and in some cases, may undergo fibrous metaplasia and produce collagen. Hydropic degeneration of epithelial cells may result in large, rounded cells known as bladder cells. Existing lens fibers may liquefy and fragment, forming characteristic globules of denatured lens proteins known as Morgagnian globules.
With their superior ability to visualize and evaluate cataracts, ophthalmologists are also able to classify cataracts in a variety of different ways, including age of onset (e.g. juvenile vs senile), anatomic location (e.g. subcapsular vs. equatorial), extent (mature vs. hypermature), or pathogenesis. Because this is a course in pathology, and not ophthalmology, we will focus primarily on classifying cataracts according to their pathophysiology, rather than through other metrics.
5.1.1 Inherited
Inherited cataracts are most commonly reported in dogs, and are relatively infrequent in other species. They may be congenital or may appear at any stage in the life of the animal. Diagnosis of an inherited cataract is based on the signalment, paying particular attention to breed predispositions, the age of presentation, and the ophthalmologic type of cataract. Histopathology alone cannot distinguish between types of cataracts.
5.1.2 Diabetic cataracts
Diabetic cataracts are one of the most frequently encountered type of cataract seen by practitioners. They are most common in dogs.
The pathogenesis of diabetic cataracts relates to the metabolism of glucose. As noted earlier, the lens absorbs glucose from the aqueous humour, and, using the anaerobic hexokinase pathway, metabolizes glucose into energy. In diabetic dogs, the concentration of glucose in the blood and aqueous is elevated, and excess glucose enters the lens. The concentration of glucose overwhelms the hexokinase pathway and is shunted into the aldose reductase pathway, which results in the production of sorbitol. Sorbitol is too large to exit the lens, and as it accumulates, it causes an increase in the osmotic pressure within the lens, leading to influx of water. The end result is hydropic rupture of lens fibers that manifests clinically as a cataract.
Microscopically, there is nothing distinctive about a diabetic cataract. The diagnosis is based on clinical signs, symptoms, diagnosis of diabetes mellitus, and ophthalmologic type of cataract.
Interestingly, it is not solely an increase in intraocular glucose that leads to cataract. It would appear that there are species differences in the amounts of aldose reductase within the lens, and it is these differences that are thought to contribute to the frequency of diabetic cataracts in different species. For example, although diabetes mellitus is relatively common in cats, diabetic cataracts are rare, because the concentration of aldose reducates within their lens is low.
5.1.3 Other causes of cataracts
There are several other causes of cataracts. Nutritional cataracts are best described in carnivores that have been fed milk replacer, but the pathogenesis is unclear.
Radiation therapy is a well-known risk factor for the development of cataracts. Cataracts may develop approximately 6-12 months post-therapy, and the risk of development is dependent on the dose received during treatment. The underlying pathogenesis relates to necrosis of the equatorial germinal lens epithelial cells.
Infectious agents may also lead to cataracts. In cattle, infection with bovine viral diarrhea virus (BVDV) in utero is associated with cataract development. In fish, infection with the fluke Diplostomum spathaceum leads to cataracts.
Finally, luxation of the lens may result in cataract through unknown means, though it is thought that disruption of nutrition is the underlying cause.
5.2 Luxation
Lens luxation (dislocation) may be complete or partial (subluxation). It is a gross or clinical diagnosis: sectioning of the globe for histologic process typically disrupts the normal anatomic position of the lens. A luxated lens may be found partially or completely within the anterior chamber, or it may remain in the posterior chamber. Displacement of the lens into the anterior chamber can disrupt and obstruct the flow of the aqueous, resulting in glaucoma.
Lens luxation may be primary or secondary. Primary lens luxations occur without any known trauma or ocular disease, and may be spontaneous or the result of inherited defects in the zonules.
More common is secondary luxation, or those with a known cause, which may include trauma, weakened zonules due to a greatly expanded glaucomatous globe, or zonules weakened secondarily to uveitis. Note that glaucoma can both cause and be the result of lens luxation, and that it can be difficult to separate cause and effect when presented with a one-time snapshot of the lesions.
5.3 Feline post-traumatic ocular sarcoma
Cats suffering trauma or damage to the lens may present months to years later with a malignant and destructive intraocular neoplasm known as feline post-traumatic ocular sarcoma. Cats typically present with a refractory uveitis, cataract, and a history of ocular trauma. The neoplasm is thought to arise from malignant transformation of the lens epithelium, possibly mirroring the pathogenesis of post-vaccinal/injection site sarcoma that is occasionally seen in cats.
Grossly, the neoplasm is grey to white and proliferative, often compresses the lens. The mass expands and grows along the circumference of the globe, and is ultimately invasive, frequently infiltrating into the optic nerve or sclera.